


 Sign Out
Sign Out



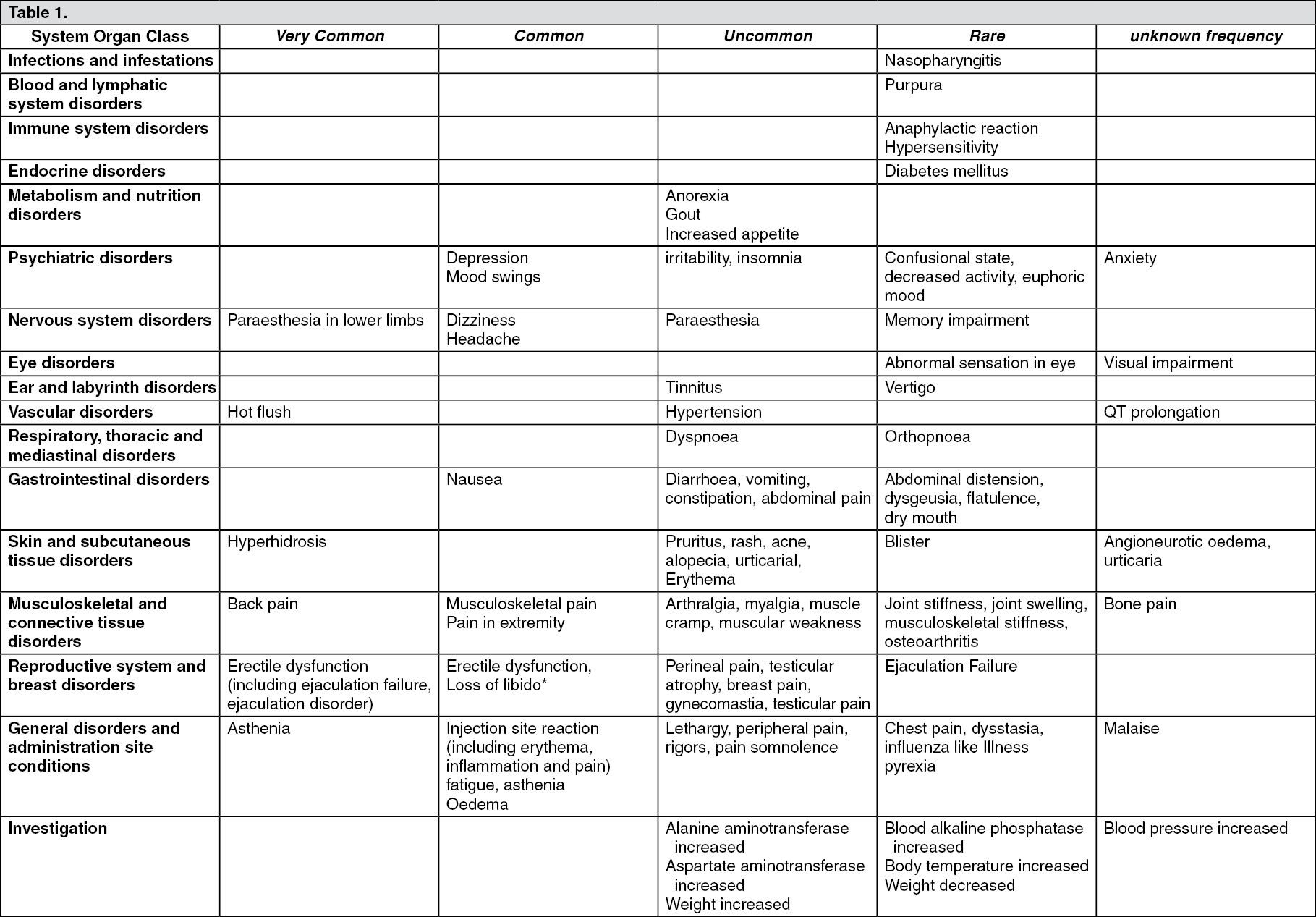
The following adverse reactions, considered as at least possibly related to triptorelin treatment, were reported. Most of these are known to be related to biochemical or surgical castration.
The frequency of the adverse reactions is classified as follows: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000). No frequency can be determined for the adverse reactions reported after marketing. Consequently, they are reported with frequency "not known".
3.75 mg: (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image11.25 mg: (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTriptorelin causes a transient increase in circulating testosterone levels within the first week after the initial injection of the sustained release formulation. With this initial increase in circulating testosterone levels, a small percentage of patients (≤ 5%) may experience a temporary worsening of signs and symptoms of their prostate cancer (tumour flare), usually manifested by an increase in urinary symptoms and metastatic pain which can be managed symptomatically. These symptoms are transient and usually disappear in one to two weeks.
Isolated cases of exacerbation of disease symptoms, either urethral obstruction or spinal cord compression by metastasis have occurred. Therefore, patients with metastatic vertebral lesions and/or with upper or lower urinary tract obstruction should be closely observed during the first few weeks of therapy.
The use of GnRH agonists, to treat prostate cancer may be associated with increased bone loss and may lead to osteoporosis and increases the risk of bone fracture.
An increase in lymphocytes has been reported in patients treated with GnRH analogues. This secondary lymphocytosis is apparently related to castration induced by GnRH and suggests that gonadal hormones are involved in thymic involution.
Patients receiving long-term treatment by GnRH analogue in combination with radiation may have more side effects especially gastrointestinal, related to radiotherapy.
General tolerance in women: As a consequence of decreased oestrogen levels, the most commonly reported adverse events (expected in 10% of women or more) were headache, libido decreased, sleep disorder, mood altered changes, dyspareunia, dysmenorrhoea, genital haemorrhage, ovarian hyperstimulation syndrome, ovarian hypertrophy, pelvic pain, abdominal pain, vulvovaginal dryness, hyperhidrosis, hot flushes.
The following adverse reactions, considered as at least possibly related to triptorelin treatment, were reported. Most of these are known to be related to biochemical or surgical castration.
3.75 mg: The frequency of the adverse reactions is classified as follows: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1000 to <1/10). No frequency can be determined for the adverse reactions reported after marketing. Consequently, they are reported with frequency "not known". (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image11.25 mg: The frequency of the adverse reactions is classified as follows: very common (≥1/10); common (≥1/100 to <1/10). No frequency can be determined for the adverse reactions reported after marketing. Consequently, they are reported with frequency "not known". (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAt the beginning of treatment, the symptoms of endometriosis including pelvic pain, dysmenorrhoea may be exacerbated very commonly (≥ 10%) during the initial transient increase in plasma oestradiol levels. These symptoms are transient and usually disappear in one or two weeks.
Genital haemorrhage including menorrhagia, metrorrhagia may occur in the month following the first injection.
Long-term use of GnRH analogues may lead to bone loss which is a risk factor of osteoporosis.
3.75 mg: When used to treat infertility, the combination with gonadotrophins may result in ovarian hyperstimulation syndrome. Ovarian hypertrophy, pelvic and/or abdominal pain may be observed.
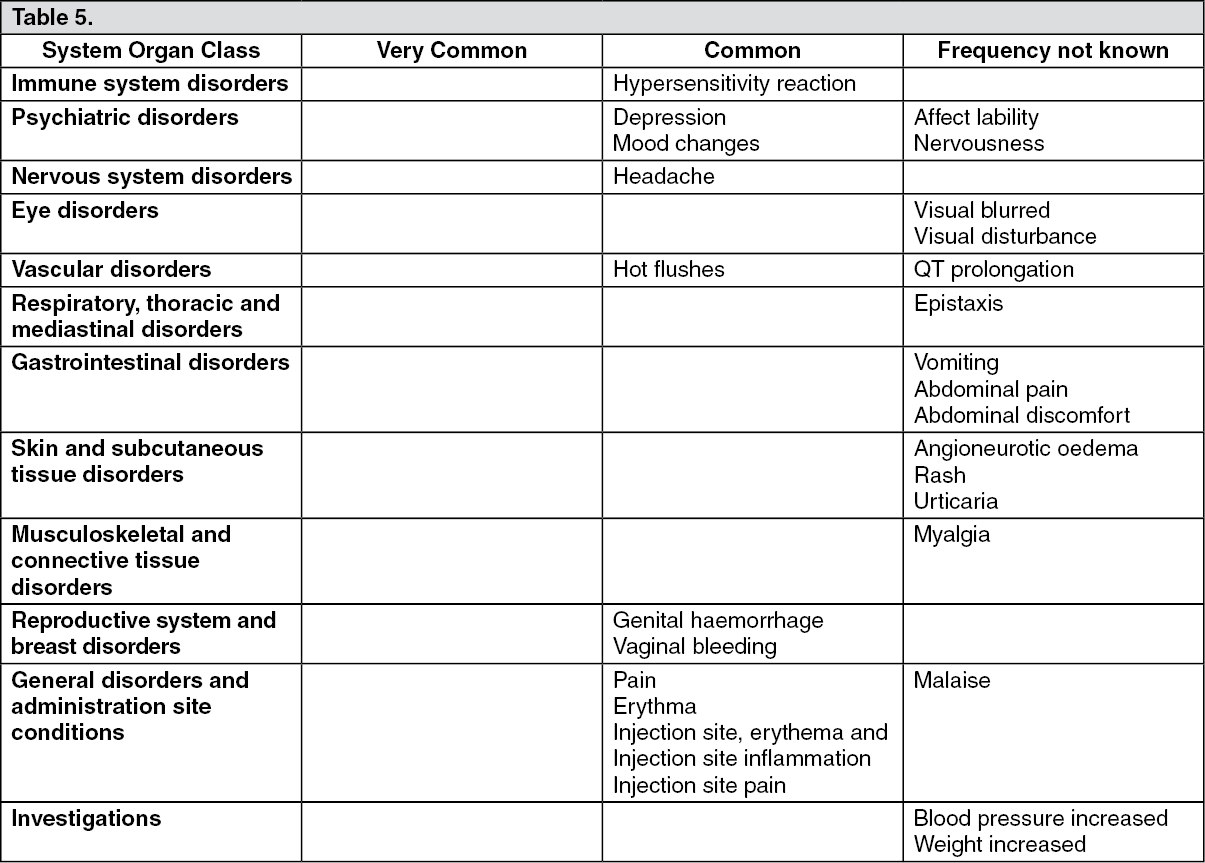
General tolerance in children: 3.75 mg: The frequency of the adverse reactions is classified as follows: very common (≥1/10); common (≥1/100 to <1/10). No frequency can be determined for the adverse reactions reported after marketing. Consequently, they are reported with frequency "not known". (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image11.25 mg: As seen with other GnRH agonist therapies, the most commonly observed adverse events related to triptorelin treatment in clinical trials were due to its expected pharmacological effects. These effects included vaginal bleeding including spotting.
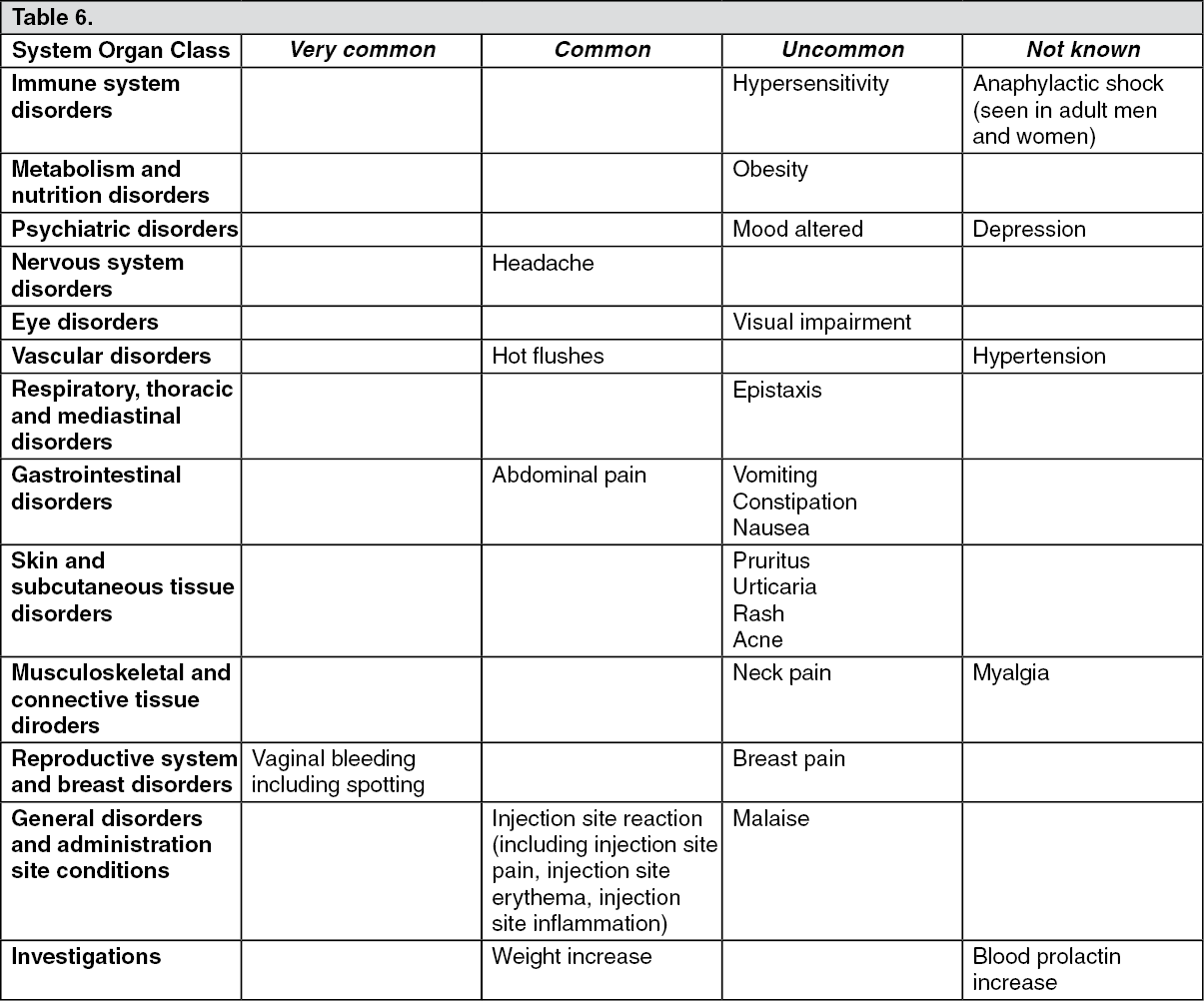
The following adverse reactions, considered as at least possibly related to triptorelin treatment, were reported.
The frequency of the adverse reactions is classified as follows: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100). No frequency can be estimated for the adverse reactions reported after marketing. Consequently they are reported with frequency "not known". (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageVaginal bleeding may occur in the month following the first injection.
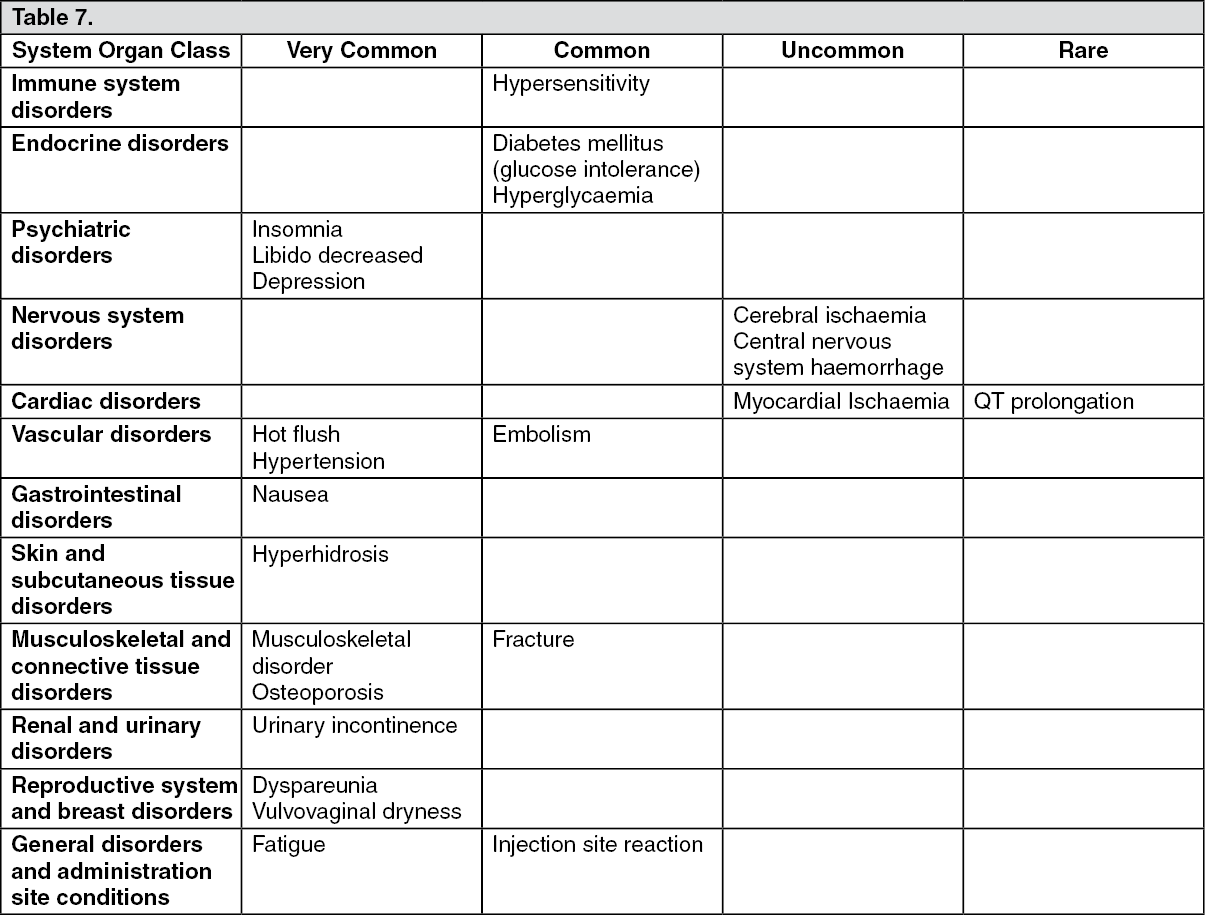
3.75 mg: Breast Cancer: The most commonly observed adverse reactions associated with triptorelin treatment for up to 5 years in combination with either tamoxifen or an aromatase inhibitor in the TEXT and SOFT studies were hot flush, musculoskeletal disorder, fatigue, insomnia, hyperhidrosis, vulvovaginal dryness and depression.
The frequencies of the adverse reactions reported with triptorelin in combination with tamoxifen (N = 2325) or exemestane (N = 2318) are shown in the Table 7. The classifications are as follows: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1000). (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe ADRs identified previously should be used in addition to the triptorelin ADRs identified in men and women in tables previously mentioned to fully describe the ADR profile for the use of OFS in combination with either exemestane or tamoxifen.
Osteoporosis has been reported with a higher frequency with the use of triptorelin in combination with exemestane than in the combination with tamoxifen (39% versus 25%).
Musculoskeletal disorder and fractures were also more commonly reported in the combination with exemestane than in the combination with tamoxifen (89% versus 76% and 6.8% versus 5.2%, respectively).
Hypertension has been reported as a targeted adverse event at a very common frequency with triptorelin in combination with either exemestane or tamoxifen (23% and 22% respectively).
Hyperglycaemia and diabetes have been reported as targeted adverse events at a common frequency with triptorelin in combination with either exemestane or tamoxifen (hyperglycaemia: 2.6% and 3.4% respectively; diabetes: 2.3% and 2.3% respectively.
View ADR Monitoring Form